Please review all the information found in this module along with the case study. Please also answer the questions at the end of this module. Following taking this web based module on arterial blood gases (ABGs) you should have learned the following:
1. To identify normal values for Arterial Blood Gases (ABG’s).
2. Be able to analyze ABG’s to help understand diagnosis and/or classification.
3. Be able to identify signs and symptoms of respiratory and metabolic acidosis and alkalosis,
1. To identify normal values for Arterial Blood Gases (ABG’s).
2. Be able to analyze ABG’s to help understand diagnosis and/or classification.
3. Be able to identify signs and symptoms of respiratory and metabolic acidosis and alkalosis,
What are ABGs
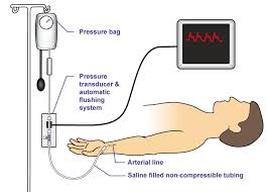
Arterial blood gases are usually obtained by placing an arterial line in the radial artery but other arteries could be used as well. An arterial line also measures SBP, DBP (nice right, so you don't need to manually take BP.
*We will be discussing ABGs from an arterial line
*PT safety note: when walking into the hospital room do a visual inspection and be aware of all the lines and tubes. From the blood the following values are obtained: pH, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), bicarbonate (HCO3) concentration and bases excess (BE).
PT Safety Note: When treating a patient within an arterial line:
Lots of values here so to help ease the reading and comprehension, click on the video on the right and enjoy the relaxing sound of the ocean.
- arterial sample is from a needle puncture or indwelling cannula in a peripheral artery
- Venous samples (VBGs) are taken from venous puncture or catheter
- mixed venous samples are taken from a pulmonary artery
*We will be discussing ABGs from an arterial line
*PT safety note: when walking into the hospital room do a visual inspection and be aware of all the lines and tubes. From the blood the following values are obtained: pH, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), bicarbonate (HCO3) concentration and bases excess (BE).
PT Safety Note: When treating a patient within an arterial line:
- Keep wrist in slight extension, avoid wrist flexion, avoid weight bearing on arm
- No ROM at site
- Make sure there is enough slack when moving patient
Lots of values here so to help ease the reading and comprehension, click on the video on the right and enjoy the relaxing sound of the ocean.
|
|
Why are they important?
An arterial blood gas report is a critical part of diagnosing and managing a patients. For example they allow us to determine a patient's oxygen status and the effectiveness of oxygen therapy. ABG report also allows us to evaluate respiratory diseases and conditions that effect the lungs as well as providing information about the body's acid/base balance.
**As Physical Therapists it is important to understand what these numbers mean to better manage physical therapy interventions especially with patients receiving mechanical ventilation and noninvasive mechanical ventilation.
Clinical Tip:
In Acute Care and ICU setting are used to assess current status as well as medical interventions. Since ABGs are often taken after the modes on the ventilator has been changed the PT may have to wait until after the ABG has been taken.
**As Physical Therapists it is important to understand what these numbers mean to better manage physical therapy interventions especially with patients receiving mechanical ventilation and noninvasive mechanical ventilation.
Clinical Tip:
In Acute Care and ICU setting are used to assess current status as well as medical interventions. Since ABGs are often taken after the modes on the ventilator has been changed the PT may have to wait until after the ABG has been taken.
Components of Arterial Blood Gases
pH
Measures acidity or alkalinity of the blood, based on the hydrogen (H+) ions. Acids give up H+ in the blood and Bases accept H+ (I am sure I am bringing back fond memories of Chem!)
Ranges from 1-14….acidic to basic.
pH <7.4 is called acidemia and the process is called acidosis. There are only two ways for acidemia to occur:
Helpful Hint: don't let the range and the normal confuse you. I will try to remember to place test questions less or greater than the range i.e., <7.35 or >7.45.
Also, no worries about the above information, since I have made figuring it easy. Trust me, you will see later on.
Ranges from 1-14….acidic to basic.
- Clinically, it provides insight to the nature and severity of the respiratory and metabolic conditions. I will discuss this topic more later on, but if you are so thrilled about this topic and can't wait, stroll down to the "Helpful Tip" section (ha).
pH <7.4 is called acidemia and the process is called acidosis. There are only two ways for acidemia to occur:
- low HCO3 (Metabolic Acidosis)
- High PaCO2 (Respiratory Acidosis, which is the same what?)
- Yes, Alveolar Hypoventilation and Hypercapnia (so smart!) Hint: I heard Dr. B tends to use these words interchangeably on exams
- High HCO3, which is called Metabolic Alkalosis
- Low PaCO2, which is called Respiratory Alkalosis; another name for this would be ____________________ and ____________?
Helpful Hint: don't let the range and the normal confuse you. I will try to remember to place test questions less or greater than the range i.e., <7.35 or >7.45.
Also, no worries about the above information, since I have made figuring it easy. Trust me, you will see later on.
PaO2
Partial pressure of oxygen dissolved in arterial blood
Normal range is 80-100 mm Hg
If below 80 mm Hg and younger than 60 years of age the patient would be considered to have hypoxemia. Hypoxemia can be defined as a decreased O2 in the arterial blood.
Other ranges for hypoxemia include:
60-80 mm Hg = mild hypoxemia
40-60 mm Hg = moderate hypoxemia
< 40 mm Hg = severe hypoxemia
PT Significance: younger healthy adults may have a PaO2 of 100% and for a healthy 70 to 80 year-old is 75-80 mm Hg.
Normal range is 80-100 mm Hg
If below 80 mm Hg and younger than 60 years of age the patient would be considered to have hypoxemia. Hypoxemia can be defined as a decreased O2 in the arterial blood.
Other ranges for hypoxemia include:
60-80 mm Hg = mild hypoxemia
40-60 mm Hg = moderate hypoxemia
< 40 mm Hg = severe hypoxemia
PT Significance: younger healthy adults may have a PaO2 of 100% and for a healthy 70 to 80 year-old is 75-80 mm Hg.
SaO2

Arterial oxygen saturation PaO2 is the percent of hemoglobin (Hb) that is fully bound to 02. and is measured from a sample of arterial blood but can also be estimated by using pulse oximetry SaO2. Normal ranges are between 95%-100 %.
Clinically, SaO2 below 90% is an indicator for oxygen therapy and for the PT to contact the PCP. SaO2 in the low 90's is not an indicator for supplemental O2 but need to be watched.
***Remember PaO2 is the not the same as SaO2
Refer to Hillegass test (page 358 and/or the article I posted) to a decision tree that is helpful regarding supplemental oxygen use with activity.
- Things to consider as a PT when using oximetry: Nail polish, dirt, blood etc should be removed on the finger being used since it may not give a recording or be accurate (blocking the sensor). Other factors where oximetry may not yield accurate results include: jaundice, anemia, low perfusion (i.e., diabetes); dysrhythmias.
- Since oximetry readings can be distorted for a variety of reasons as mentioned above, correlate HR readings from the oximeter to manual readings when you are presented with an "unusual number"
- Remember that even hospital quality oximeters have a +/- 2% error within the 90%-100% range and a +/- of 3% error in the 80-90% range.
- Place on third or 4th finger
- SaO2 less than 90%
Clinically, SaO2 below 90% is an indicator for oxygen therapy and for the PT to contact the PCP. SaO2 in the low 90's is not an indicator for supplemental O2 but need to be watched.
***Remember PaO2 is the not the same as SaO2
Refer to Hillegass test (page 358 and/or the article I posted) to a decision tree that is helpful regarding supplemental oxygen use with activity.
PaCO2
Amount of carbon dioxide dissolved in arterial blood with a normal range being 35-45 mm Hg.
Question: What is occurring when CO2 is below 35 mm Hg?
Answer: Patient is hyperventilating (increased ventilation) and blowing off more CO2 than normal.
Question: What is occurring when CO2 is greater than 45 mm Hg?
Answer: Patient is hypoventilating (decreased alveolar ventilation) and not blowing off as much as CO2 as normal.
Question: If a patient's PaCo2 is greater than 50 mm Hg, what condition would they most likely have
Answer: I am hoping someone will ask this in class, since it will tell me that at least one person has reviewed this (in between studying for Ortho) and since it sounds like a good test question.
Clinically Which type of patients would you expect to be have a below normal PaCO2 value?
Answer: Patients with anxiety, nervousness, heart failure, side effect of drugs, severe pain, stress.
Clinically Which type of patients would you expect to have an increased in arterial CO2?
Answer: Patients with COPD
Question: What is occurring when CO2 is below 35 mm Hg?
Answer: Patient is hyperventilating (increased ventilation) and blowing off more CO2 than normal.
Question: What is occurring when CO2 is greater than 45 mm Hg?
Answer: Patient is hypoventilating (decreased alveolar ventilation) and not blowing off as much as CO2 as normal.
Question: If a patient's PaCo2 is greater than 50 mm Hg, what condition would they most likely have
Answer: I am hoping someone will ask this in class, since it will tell me that at least one person has reviewed this (in between studying for Ortho) and since it sounds like a good test question.
Clinically Which type of patients would you expect to be have a below normal PaCO2 value?
Answer: Patients with anxiety, nervousness, heart failure, side effect of drugs, severe pain, stress.
Clinically Which type of patients would you expect to have an increased in arterial CO2?
Answer: Patients with COPD
HCO3
Calculated value of the amount of bicarbonate in bloodstream
Normal range: 22-26 mEq/liter
Below 22= acidic
Above 26= alkalotic
Normal range: 22-26 mEq/liter
Below 22= acidic
Above 26= alkalotic
Other measurements obtained by an arterial line
Hemoglobin (Hgb): Normal range: 12 to 16 g/100ml
Males: 14-17 Gm/dL
Females: 12-16 Gm/dL
Question: Which patients are susceptible to low levels of Hgb?
Answer: Post surgical patients i.e., joint replacements and patients with advanced COPD.
Signs and symptoms for a patient with low hemoglobin include fatigue and weakness.
B.E./B.D.
Indicates amount of excess or insufficient level of bicarbonate in the system. Negative indicates base deficit (B.D. and Positive indicates base excess B.E.)).
Normal range: -2 to +2 mEq/liter
*** The B.E./B.D report along with the pH helps determine whether the person is in an acute stage or chronic stage. If pH is not in the normal range of 7.35 to 7.45 the patient is in an acute stage but as he/she moves towards normal it's considered partially compensated and when normal it's considered chronic (completely compensated). The therapist can determine this by looking at a series of ABG reports.
Lets look at an example!
A patient with a dx of COPD and has CO2 of 48 mm Hg (yes, difficulty blowing off CO2, thus retaining more that he should) has a pH of 7.25?
Question: Would you say he is in an acute or chronic stage?
Answer: If you said chronic, you are wrong; correct answer is acute.
OK, Next Question: OK, how about at the next ABG report the pH indicates 7.30. Would you say acute, partially compensated or fully compensated?
Answer: Yes! You are correct the answer is partially compensated since the body is obtaining more base (most likely +3) to move the pH closer to normal.
Last Question: Next ABG report comes back and pH is normal (7.35) with the PCO2 of 55 mm Hg. Acute, partially compensated, or chronic (completely compensated)?
Answer: Perfect! yes, chronic! OK, now go take a break!!
Males: 14-17 Gm/dL
Females: 12-16 Gm/dL
Question: Which patients are susceptible to low levels of Hgb?
Answer: Post surgical patients i.e., joint replacements and patients with advanced COPD.
Signs and symptoms for a patient with low hemoglobin include fatigue and weakness.
B.E./B.D.
Indicates amount of excess or insufficient level of bicarbonate in the system. Negative indicates base deficit (B.D. and Positive indicates base excess B.E.)).
Normal range: -2 to +2 mEq/liter
*** The B.E./B.D report along with the pH helps determine whether the person is in an acute stage or chronic stage. If pH is not in the normal range of 7.35 to 7.45 the patient is in an acute stage but as he/she moves towards normal it's considered partially compensated and when normal it's considered chronic (completely compensated). The therapist can determine this by looking at a series of ABG reports.
Lets look at an example!
A patient with a dx of COPD and has CO2 of 48 mm Hg (yes, difficulty blowing off CO2, thus retaining more that he should) has a pH of 7.25?
Question: Would you say he is in an acute or chronic stage?
Answer: If you said chronic, you are wrong; correct answer is acute.
OK, Next Question: OK, how about at the next ABG report the pH indicates 7.30. Would you say acute, partially compensated or fully compensated?
Answer: Yes! You are correct the answer is partially compensated since the body is obtaining more base (most likely +3) to move the pH closer to normal.
Last Question: Next ABG report comes back and pH is normal (7.35) with the PCO2 of 55 mm Hg. Acute, partially compensated, or chronic (completely compensated)?
Answer: Perfect! yes, chronic! OK, now go take a break!!
Helpful Tip on how to figure out whether Respiratory or Metabolic Conditions
Interpretation of ABGs to determine Respiratory vs. Metabolic
1.Determine if pH represents acidemia or alkalemia
2.Determine relationship between pH and CO2.
Less than 30 mm Hg= alveolar hyperventilation
Between 30-50 mm Hg adequate alveolar ventilation
>50 mm Hg= Ventilatory failure
Think you have it? Let's try some examples!
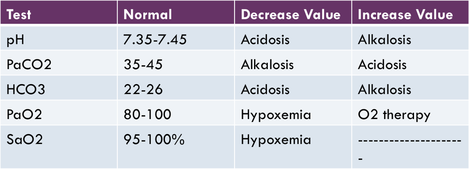
**Correction on the chart above below 90% SaO2 would be considered hypoxic
1.Determine if pH represents acidemia or alkalemia
2.Determine relationship between pH and CO2.
- If normal inverse relationship between pH and PaCO2 is preserved= Respiratory issue.
- if they have a direct relationship= most likely a Metabolic Issue
Less than 30 mm Hg= alveolar hyperventilation
Between 30-50 mm Hg adequate alveolar ventilation
>50 mm Hg= Ventilatory failure
Think you have it? Let's try some examples!
**Correction on the chart above below 90% SaO2 would be considered hypoxic
Sample #1
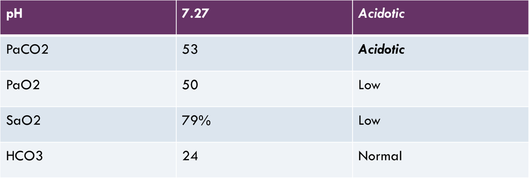
pH= acidotic and CO2= acidotic therefore the pt would be diagnosed with Respiratory Acidosis. (PaCO2 and pH has an inverse relationship so respiratory)
Clinical Tip
If working with a patient on ventilatory support (either mechanical or noninvasive) ABG is usually taken after the nurse or respiratory therapist changes the mode; so you may have to wait to start treatment until they are don.
Venous Blood Gases (VBGs) are obtained from a venous site, peripheral or central. It doesn't provide info on pH and PaCO2 and represents values from the whole body as blood returns to the heart. Generally, PCO2 from VBG is 4-8 mm Hg greater than the pure arterial sample.
Venous Blood Gases (VBGs) are obtained from a venous site, peripheral or central. It doesn't provide info on pH and PaCO2 and represents values from the whole body as blood returns to the heart. Generally, PCO2 from VBG is 4-8 mm Hg greater than the pure arterial sample.
