Welcome to Pulmonary Function Tests!
Pulmonary Function Tests is not the most exciting topic, however there are key concepts that are important for physical therapists. In this module I am hoping you achieve the following learning objectives:
- Describe the differences between different pulmonary function tests and lung capacities.
- To compare and contrast lung volumes and lung capacities between obstructive and restrictive lung dysfunctions.
- To examine pulmonary function values to help determine a likely diagnoses.
- To identify common aging changes in the lungs and thoracic cavity.
Spirometry
Here are some key things you should know about spirometry testing
- Patients wears a nose clip and is asked to inhale slowly but to maximal inspiration and then are asked to exhale as quickly and forcefully as possible.
- The patient is asked to do this 3x
- If an obstructive lung disease is suspected the patient takes a bronchodilator (albuterol), waits about 15 minutes and re-takes the test; if values improve (12% or greater), asthma is suspected
- The values (Predicted Values) are based on research norms for race, height, sex, ethnicity, and age; meaning your values (Observed Values) are compared to individuals who are similar but considered normal (volumes decrease with age, males have larger volumes than females, tall individuals have larger volumes than short individuals, American Indians, Blacks, and Asians have as much as 12-14% decrease in lung volumes than whites (Hillegass).
- Interpretation: Dividing the observed value by the predicted value= the percentage of predicted values. *Generally there needs to be 20% difference between the predicted and observed to be considered abnormal (obstructive or restrictive).
- Well the significance is that reduced lung function is a risk factor for cardiovascular mortality and reduced health status.
- Pulmonary Function tests can show how a patient is improving or regressing.
- May be helpful to show smokers how they have reduced lung function to assist them in quitting. Additionally, due to the aging population and the increase in co-morbidities a preoperative pulmonary screening is recommended. Preoperative screening can predict postoperative pulmonary complications.
OK, Time To Learn Some of the Common Terms Used for Spirometry!
In general you should think of spirometry as an instrument that measures forced expiratory volumes. Four of the most common terms you need to know and often read in the literature (I know, you are probably saying "Not sure what you are reading Professor Bartlett, but most of my reading never involves air flow measurements") are as follows:
Forced Vital Capacity (FVC) can be defined as total volume of air exhaled with maximal forced expiratory effort after a full inspiration. Clinically, when we test this on our patients, and we will do this in class using a hand-held spirometer that measures FVC, make sure you educate your patient on how to take a large inspiratory breath in (eyes up, trunk extension, then forward flexion with contraction of abdominal when exhaling. Also, clinically, FVC should be greater than or equal to 80% than their predicted norm . To look at norms for FVC go to www.osha.gov then input 1910.1043 App C in the search box (one bad thing is norms have not been updated for some time.
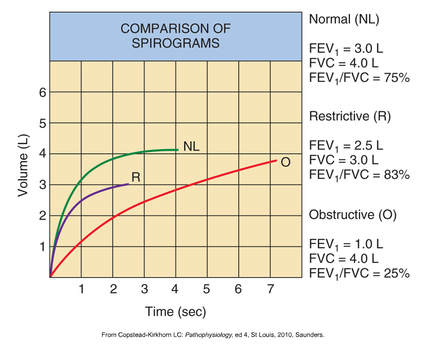
***This may be a little confusing but FVC may be normal for an individuals with an obstructive lung disease as long as they have time to empty their lungs (look at the chart to the right, you can see volume is almost at the same level of the normal individual, however look at how long it took). But what do you think happens in restrictive? Please ask me this in class, if you are not sure, plus it will show that at least one person is reading this, Ha.
Please take a second or two to review the graph to the right.
The primary difference between the curve in the individual with restrictive lung dysfunction compared to obstructive is the slope of the curve. In restrictive the person exhales most of their air within the first second. Also, look at the volume of air; quite reduced (about 3.0 L) as compared to 4.0 L); less volume (sounds familiar?).
Clinical Tip:
Individuals with restrictive lung dysfunction will have reduced lung volumes and reduced FVC due to decreased respiratory mm strength (i.e., pneumonia, IPF)
Forced Expiratory Volume in one second (FEV1) is defined as the volume of air expired during the first second during a forced vital capacity maneuver. Below is a simple relationship with FEV1 and the amount of obstruction (please look at the graph above to assist you).
The Ratio of FEV1/FVC for Normal Population: Usually 75% (meaning most individuals are able to exhale 75% of the FVC within one second.
The Ratio of FEV1/FVC Restrictive: If greater than 80 to 90 percent would indicate restrictive. Check out graph above to better understand why this is the case. Basically it means that most of these individuals exhale most of their entire reduced volume within the first second. (less air in and less air out). On the other hand if the ratio (percent) is reduced it indicates an obstructive.
The Ratio of FEV1/FVC for Obstructive So here is information that will help diagnose and categorize an individual who is suspected to have COPD when performing spirometry using forced expiratory volume:
In order to stage an individual with COPD:
- Forced Vital Capacity (FVC)
- Forced Expiratory Volume in one second (FEV1)
- Ratio of FEV1/FVC
- Peak Expiratory Flow Rate (PRFR)
Forced Vital Capacity (FVC) can be defined as total volume of air exhaled with maximal forced expiratory effort after a full inspiration. Clinically, when we test this on our patients, and we will do this in class using a hand-held spirometer that measures FVC, make sure you educate your patient on how to take a large inspiratory breath in (eyes up, trunk extension, then forward flexion with contraction of abdominal when exhaling. Also, clinically, FVC should be greater than or equal to 80% than their predicted norm . To look at norms for FVC go to www.osha.gov then input 1910.1043 App C in the search box (one bad thing is norms have not been updated for some time.
***This may be a little confusing but FVC may be normal for an individuals with an obstructive lung disease as long as they have time to empty their lungs (look at the chart to the right, you can see volume is almost at the same level of the normal individual, however look at how long it took). But what do you think happens in restrictive? Please ask me this in class, if you are not sure, plus it will show that at least one person is reading this, Ha.
Please take a second or two to review the graph to the right.
The primary difference between the curve in the individual with restrictive lung dysfunction compared to obstructive is the slope of the curve. In restrictive the person exhales most of their air within the first second. Also, look at the volume of air; quite reduced (about 3.0 L) as compared to 4.0 L); less volume (sounds familiar?).
Clinical Tip:
Individuals with restrictive lung dysfunction will have reduced lung volumes and reduced FVC due to decreased respiratory mm strength (i.e., pneumonia, IPF)
- Now look at the red line (obstructive); not much air is blown out during the first second (why) but if you give the person enough time i.e., 7 seconds the person is able to blow out about 4.0 L.
Forced Expiratory Volume in one second (FEV1) is defined as the volume of air expired during the first second during a forced vital capacity maneuver. Below is a simple relationship with FEV1 and the amount of obstruction (please look at the graph above to assist you).
- little to know obstruction if FEV1 is greater than 2.0 L to normal
- Mild to moderate obstruction: FEV1 between 1.0 and 2.0 L
- Severe obstruction: FEV1 less than 1.0 L
The Ratio of FEV1/FVC for Normal Population: Usually 75% (meaning most individuals are able to exhale 75% of the FVC within one second.
The Ratio of FEV1/FVC Restrictive: If greater than 80 to 90 percent would indicate restrictive. Check out graph above to better understand why this is the case. Basically it means that most of these individuals exhale most of their entire reduced volume within the first second. (less air in and less air out). On the other hand if the ratio (percent) is reduced it indicates an obstructive.
The Ratio of FEV1/FVC for Obstructive So here is information that will help diagnose and categorize an individual who is suspected to have COPD when performing spirometry using forced expiratory volume:
In order to stage an individual with COPD:
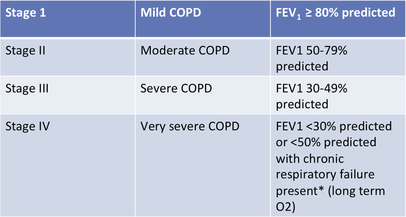
- The FEV1/FVC ratio has to be less than 70%
- Then you can use the GOLD (Global Initiative for Chronic Obstructive Lung Disease) to classify based on FEV1. Please see chart below.
Peak Expiratory Flow Rate (PEFR) is the highest flow rate achieved during a forced expiratory maneuver. This is estimated by a handheld flow meter. Clinically, PEFR determines how fast a patient can exhale and is often used for patients with asthma.


|
In using a peak flow meter the individual with asthma performs the maneuver when he/she is doing well in order to get a reading of their best performance, which can be used to compare against when they are not doing well with their asthma. The flow meter then provides them guidance on what to do based on their readings. Fore example:
|

Restrictive Lung Pathology:
OK, we have looked at some of the key characteristics that help dx and categorize someone with an obstructive lung disease (if you forgot, please scroll back up and review since you will see questions on your exam) so now lets looks at how we can determine if a person has a restrictive lung pathology. I hinted on one characteristic earlier but let's discuss it again. Remember what we discussed in class, someone with a restrictive issue they have difficulty with what? Yes, getting air into the lungs (so smart!; maybe you deserve a break! Go get some coffee and something to eat.
Welcome back! Now let's go back to restrictive lung disease. Here is what you need to know to help determine if a person has a restrictive lung impairment when doing spirometry-forced expiratory volumes; they would most likely have:
- Reduced lung capacity
- Reduced FVC
- Normal FEV1
- Most likely an above normal percent of FEV1/FVC i.e., more than 80-90%
- *** Easiest way to remember is the above is these individuals have difficulty getting air in so that would mean they have less air to come out (makes sense?) If not, place your hands on your rib cage, now squeeze real tight and try to take a real deep breath in (not much air going in right?, well if you have restriction then less air in thus less air out)
Lung Volumes and Lung Capacities
- 2nd most popular pulmonary function tests performed but they require sophisticated equipment to measure the amount of air in the lungs after a maximal expiration usually by a helium dilution technique or other expensive method used in research labs.
- Tidal Volume (VT)
- Inspiratory Reserve Volume (IRV)
- Expiratory Reserve Volume (ERV)
- Residual Volume (RV)
- Anatomic Dead Space
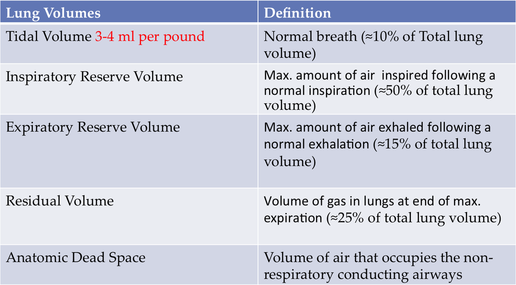

The first four lung volumes are for the most part self-explanatory but we will probably discuss more in class. However, anatomic dead space can be somewhat confusing. The best way to think of the anatomic dead space is just that " it is space within our airway conducting system that is dead, meaning it doesn't participate in gas exchange" but we have to get air passed this area to reach the alveoli so gas exchange can occur. Maybe an even better way to think of "anatomic dead space" is it being a road block that stands in your way to your favorite restaurant etc on Alexander St. (ha) and you are going to get through it with your car because you have to get there. Enough of my tangent , anatomic dead space is the volume in the non-conducting airways (trachea down to the terminal branches of the bronchi) that the air needs to get passed to reach the alveoli;*** and it is proportion to a person's body weight.
For example, my weight is about #175 so my anatomic dead space is 175 ml (yes, in general dead space corresponds to your body weight.
So, what is the big deal? An individual's tidal volume (normal breath) needs to be large enough to get past the anatomic dead space to reach the alveoli; the O2 that reaches the alveoli is considered alveolar ventilation. Now, let's continue our example; an average TV (normal breath in) is about 500 ml for an adult. But if we use my weight as an example and the average TV is 3.5 ml (see chart above) my tidal volume would be roughly 612 ml. So, what is my alveolar ventilation per breath? So smart! yes 437 ml (612-175). If we want to calculate alveolar ventilation per minute we would use the following formula: AV=(VT x RR) - VD x RR)
AV = alveolar ventilation ml/min
VT = Tidal volume ml/min
RR = respiratory rate
VD = Dead space ml/min
So calculate my alveolar ventilation per minute if my RR = 15
AV= ( 612 x 15) - (175 x 15)
AV = 9,180 - 2625
AV = 6,555 ml or 6.5 L
*Normal values are about 4-5 L for an adult
Yikes; Is this getting confusing? Well, let's think about our patients with neurological impairments? How do they often present (did you assess their breathing pattern). "Yes, Professor Bartlett, I am taking what I learn in your class and carrying it over to the clinic" (what great students) Yes, many have limited tidal volume due to them breathing in a shallow pattern.
Clinical Significance:
Question: What happens when a person has a decreased tidal volume? Yes, the person has to work harder (increased RR) to get enough air to the alveoli thus causing fatigue. Work of breathing can be defined as minute ventilation (MV) with MV = TV X RR. Besides patients with neurological impairments or neuromuscular weakness, what other conditions can cause an individual not to reach normal TV? Right again! individuals who had a surgical procedure, rib fractures, even someone wearing a TLSO could cause decreased TV.
All right! enough of the anatomic dead space. But before we move on to lung capacity we need to take a quick look at residual volume (air remaining in the lungs after maximal expiration). A person with an obstructive lung disease would most likely have an increase in residual volume (makes sense right since we know these individuals have difficulty getting air out). In restrictive patterns there may be a decrease in RV (since they have more difficulty getting air in, they would automatically have decreased RV) and may increase the risk for a the lung to collapse. Yes, RV is important to keep the lungs from collapsing.
For example, my weight is about #175 so my anatomic dead space is 175 ml (yes, in general dead space corresponds to your body weight.
So, what is the big deal? An individual's tidal volume (normal breath) needs to be large enough to get past the anatomic dead space to reach the alveoli; the O2 that reaches the alveoli is considered alveolar ventilation. Now, let's continue our example; an average TV (normal breath in) is about 500 ml for an adult. But if we use my weight as an example and the average TV is 3.5 ml (see chart above) my tidal volume would be roughly 612 ml. So, what is my alveolar ventilation per breath? So smart! yes 437 ml (612-175). If we want to calculate alveolar ventilation per minute we would use the following formula: AV=(VT x RR) - VD x RR)
AV = alveolar ventilation ml/min
VT = Tidal volume ml/min
RR = respiratory rate
VD = Dead space ml/min
So calculate my alveolar ventilation per minute if my RR = 15
AV= ( 612 x 15) - (175 x 15)
AV = 9,180 - 2625
AV = 6,555 ml or 6.5 L
*Normal values are about 4-5 L for an adult
Yikes; Is this getting confusing? Well, let's think about our patients with neurological impairments? How do they often present (did you assess their breathing pattern). "Yes, Professor Bartlett, I am taking what I learn in your class and carrying it over to the clinic" (what great students) Yes, many have limited tidal volume due to them breathing in a shallow pattern.
Clinical Significance:
Question: What happens when a person has a decreased tidal volume? Yes, the person has to work harder (increased RR) to get enough air to the alveoli thus causing fatigue. Work of breathing can be defined as minute ventilation (MV) with MV = TV X RR. Besides patients with neurological impairments or neuromuscular weakness, what other conditions can cause an individual not to reach normal TV? Right again! individuals who had a surgical procedure, rib fractures, even someone wearing a TLSO could cause decreased TV.
All right! enough of the anatomic dead space. But before we move on to lung capacity we need to take a quick look at residual volume (air remaining in the lungs after maximal expiration). A person with an obstructive lung disease would most likely have an increase in residual volume (makes sense right since we know these individuals have difficulty getting air out). In restrictive patterns there may be a decrease in RV (since they have more difficulty getting air in, they would automatically have decreased RV) and may increase the risk for a the lung to collapse. Yes, RV is important to keep the lungs from collapsing.
Lung Capacities
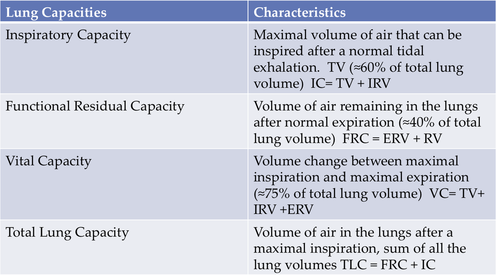
Not that the first three lung capacities are not important but I would like you to focus on total lung volume. Total lung volume is how the American Thoracic Society categorizes someone with a restrictive lung disease. Please see the chart below.
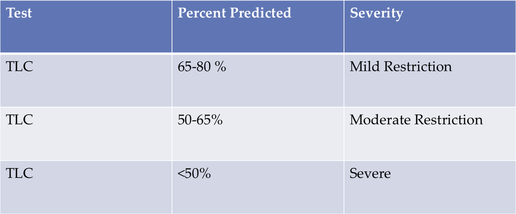
*** unlike someone with a restrictive disease, who would have decreased lung capacity, someone with COPD may have normal or above average TLC greater than 100% predicted.
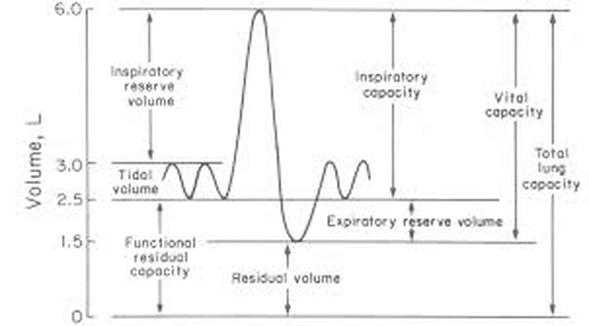
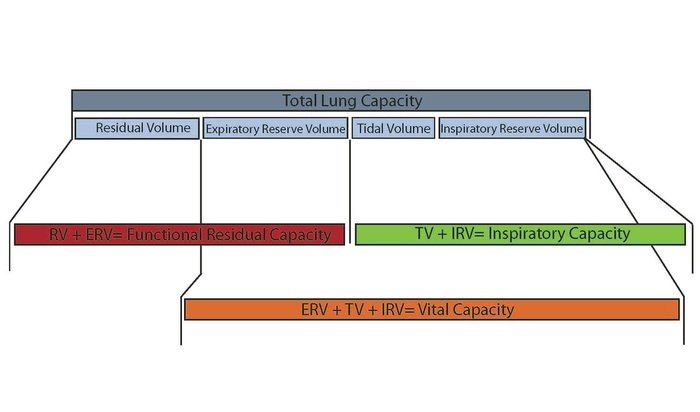
I am sure at this point you are having difficulty keeping track of all the lung volumes, lung capacities etc. Below is a few different diagrams that may help you remember the lung capacities.
I am sure at this point you are having difficulty keeping track of all the lung volumes, lung capacities etc. Below is a few different diagrams that may help you remember the lung capacities.
Aging Changes in the Lungs
Changes
References
- Ribcage changes-bones get thinner and rigid
- Muscles become weaker
- Alveoli lose their shape
- Ossification of costal and vertebral cartilage
- Average decline in FEV1 is 40 mL per year for men and 30 mL for women
- Individual with COPD may have a decline of 50-80 mL per year
- A significant decline in FEV1 is associated with higher all-cause mortality rates among both males and females (Hillegass)
- Increased risk for lung infections (pneumonia, bronchitis)
- Shortness of breath
- Decrease O2 sats
- Abnormal breathing patterns
- Exercise, breathing exercises, keep individuals active, positioning
References
Hillegass Ellen. Essentials of Cardiopulmonary Physical Therapy 4th ed. St. Louis, Missouri : Elsevier Inc. 2017:346-352
